

Video could not be played
Department of Pathology
Overview
Our faculty and trainees hail from different cultures, backgrounds and communities in the New York metropolitan area, across the United States and around the world. They come together in a shared spirit of collegiality, collaboration, and dedication to improving human health through the pursuit of clinical, scientific, and academic excellence.
Education Training Programs
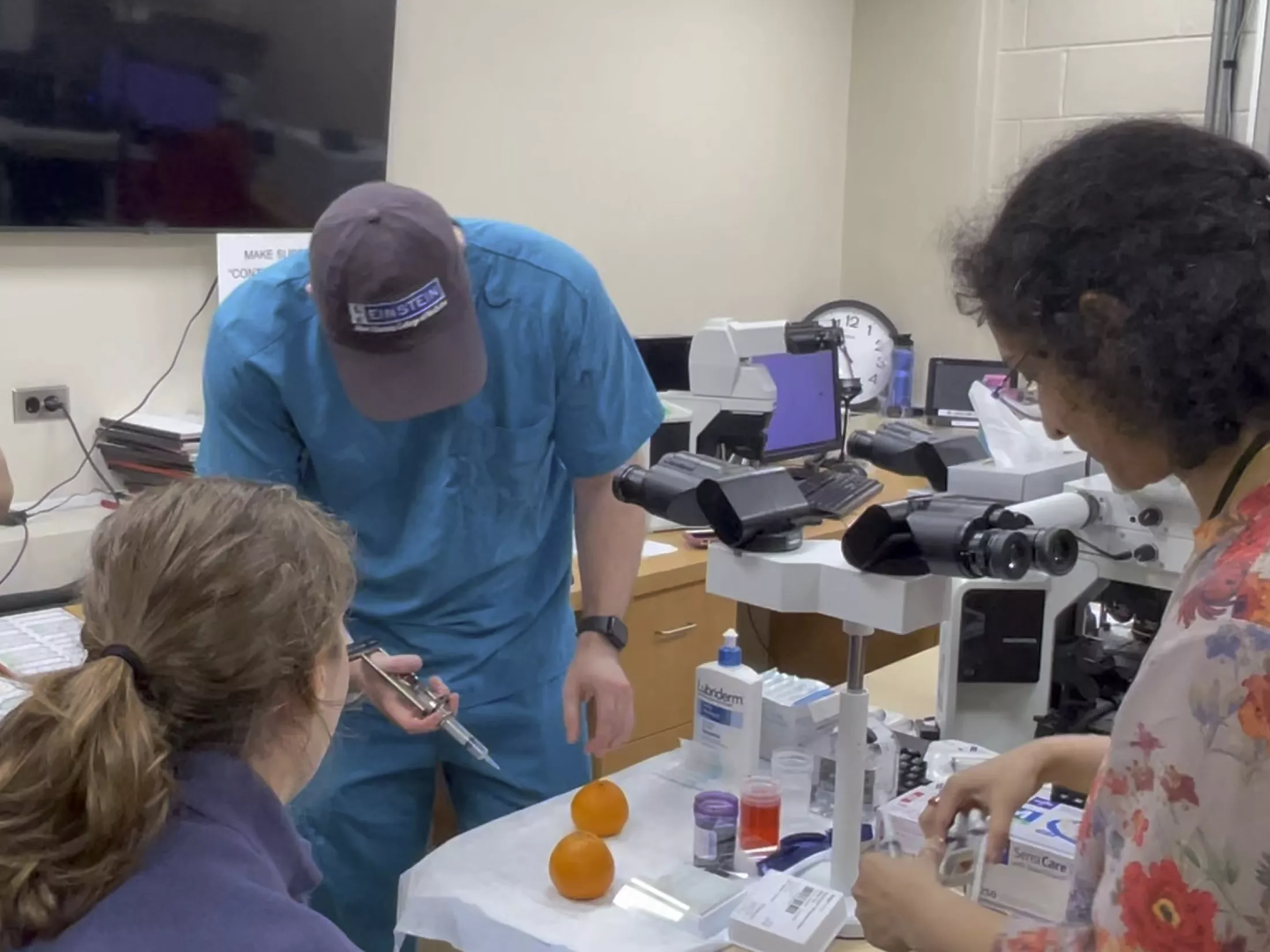
The Montefiore Einstein Department of Pathology is home to approximately 20 residents, 8 clinical fellows, 15 postdoctoral scholars, and 15 graduate students, including candidates enrolled in Einstein’s Medical Scientist Training Program.
Our clinical residents and fellows receive their training from expert pathologists representing a broad range of subspecialties. On the research side, trainees are mentored by world-class scientists.

Video could not be played
Residency Program
Video could not be played
Fellowship Program
Video could not be played
Ph.D. Program

Video could not be played
Medical Education


Video could not be played
The Scope Newsletter
Trending @EinsteinPath
Contact Us
-
Albert Einstein College of Medicine
Jack and Pearl Resnick Campus
1300 Morris Park Avenue
Belfer Building, Room 713
Bronx, NY 10461 -
erika.urie@einsteinmed.edu
-
718-430-2828
-
All Office Contacts
